MIMI® Minimally Invasive Method of Implantation - FAQ
 Since when has MIMI® been applied?
Since when has MIMI® been applied?
MIMI® has been applied for over 30 years! When proceeding according to the patient-friendly "keyhole surgery", the diameter of the drilled bone cavity is to be smaller than the diameter of the implant thread. At the beginning, the drilling is to be carried out with triangular drills (and not with cylindrical drills). Unlike previous assumptions, studies over the last decade have shown that there is no risk of "connective tissue encapsulation" around implants because of the possible penetration of "mucosa cells" into the small bone cavity and that there is no risk of "losing bone cells due to a bone compression". As a rule, you can drill the bone cavity transgingivally, which means through the gingiva. A tooth extraction can often be more uncomfortable for patients than a MIMI® implantation. Dr. Armin Nedjat, the developer of the Champions® implants system and the president of the association of innovative-practicing dentists, the "VIP-ZM" (in German: "Verein der innovativ-praktizierenden Zahnmediziner/innen e.V"), has established the MIMI® treatment that has been incorporated into standard Implantology since about 1997!
 What is the success prognosis of MIMI®?
What is the success prognosis of MIMI®?
The MIMI® success prognoses are - considering the correct indications, procedures and prosthodontic concepts - at least consistent with those of the CIM, the Classical Implantation Method (with standard incisions and flaps) and in the opinion of many implant users worldwide, the MIMI® method has more advantages than the CIM method! With the keyhole surgery, there is a lower risk of infection than with certain other surgery methods. Providing optimal care for our patients is our priority. Patients must be informed of therapy alternatives (for instance, conventional implantation methods), risks and costs. They will be provided with reliable and long-term biocompatible prosthodontic restorations!
Thanks to the MIMI® implantation technique, complicated and time-consuming bone augmentations can often be avoided, even if they might be necessary only in few cases. By applying a special technique, indirect sinus lifts can be performed over the approx. 1.3 mm - diameter drilled sockets to augment bone to approx. 2-3 mm in height. In a few cases, these bone augmentations cannot be avoided. For a good diagnosis and a clarification for patients, a 3-dimensional X-ray DVT (Digital Volume Tomography) can be necessary (costs: approx. 150 Euro), which prevents the patient from being exposed to high levels of radiation. With a DVT diagnosis, "navigation-guided implantations" can be performed using surgical templates. As a patient, you are entitled to receive comprehensive information about risks and therapy alternatives.
 Can bone augmentations always be avoided when implanting according to the MIMI® method?
Can bone augmentations always be avoided when implanting according to the MIMI® method?
No, you cannot always avoid bone augmentations when implanting according to the MIMI® method because if there is really not enough bone, you cannot perform a minimally invasive implantation. However, thanks to the MIMI technique, you can avoid extensive bone augmentations in many cases. By applying a special technique, indirect sinus lifts can be performed over the approx. 1.3 mm - diameter drilled sockets to augment bone to approx. 2-3 mm in height. In fact, you cannot always avoid bone augmentations.
 Are ceramic implants suitable for MIMI®?
Are ceramic implants suitable for MIMI®?
Zirconia, ZrO2, has been the boom material in Dental Technology in the last years. However, in the 70's, aluminium oxide ceramic implants, which- even though they had been strongly anchored in the bone for years -got fractured due to overloading of the bone. As opposed to metals and alloys, ceramic gets worn!
Zircon is likely to lose half of its strength after six years. Although no long-term experiences have been documented with zircon implants, sterile titanium, Grade IV, is recommended as material for implants. According to studies of material, it has been shown that sterile titanium, Grade IV, is one of the most stable and biologically and immunologically compatible types of materials for dental implants (Information of 1 March 2011).
 Function & MIMI® procedure
Function & MIMI® procedure
 |
 |
 |
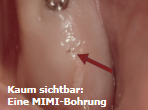
The MIMI® implantation method is based on current findings on bone physiology, according to which bone does not only tolerate compression but even needs "progressive training": preferably, without incising the mucosa and injuring the periost, a small bone cavity is drilled through the gingiva ("transgingivally"). The diameter of the bone cavity is smaller than the implant thread that will be inserted. Then, the slightly conical implant is inserted with controlled force, allowing the peri- implant bone to be laterally condensed. In this way, the implant can be completely osseointegrated.
 |
 |
 |
 Primary stability, immediate restoration & immediate loading
Primary stability, immediate restoration & immediate loading
Primary stability is one of the most important success criteria of an implant treatment. The supraconstruction should be fitted either within the first 3 to 12 days after implantation or 4-8 weeks after implantation. Preferably, the supraconstruction should be-at least partially-splinted because the 2nd to 8th weeks following surgery are the most critical concerning primary and secondary stability of the implants. You can almost always restore implants immediately, and implants can often be immediately loaded with final prosthodontic restorations on several splinted implants/teeth. Of course, the treatment depends on each individual patient case, and it is discussed with your dentist/oral surgeon practice/dental clinic. When inserting one-piece Champions to replace a single tooth, the implant can be restored immediately and eventually temporarily splinted with the adjacent teeth, the inner side surfaces of the adjacent crowns, for at least eight weeks. When splinted, there should not be any contact (even if there are side and front movements), allowing transition from primary stability to secondary stability. The patient should participate well, especially in the case of single- tooth implantations and one-piece implants (if the implant head sticks out more than 3 mm from the gingiva). The temporary restorations should not be overloaded. The patient should just eat food that he/she can break down with the tongue.
If a temporary restoration for a single tooth gets broken within the 2-8 weeks after implantation, there will be a risk of losing the implant. That is why the diagram that shows the critical osseointegration phase should be taken into consideration, and patients should participate to ensure a successful restoration!




The non-cemented temporary restoration is made and temporarily glued intra-orally on the zircon Prep-Cap (or on the titanium implant). Eight weeks later, the shaped temporary restoration - with no contact - is removed, the impression taken, and then the final crown is cemented a few days later.




Why is MIMI® so excellent, successful and why has MIMI® become the implantation method of choice?
This is due to the fact that complications can often be avoided, that the surgery is virtually bloodless, and that the tissue is protected to the maximum.








The implant is carefully and slowly inserted in the small bone cavity. First, it is inserted manually, then with a controlled torque. The patient will just feel a little bit of pressure in the bone. A source on whether the implant is anchored optimally into bone is a checking by means of a percussion sound. Should the percussion sound be bright, the implant is surrounded on all sides by bone. This can also decide on whether implants or splinted implants can be immediately loaded.


You can fit zircon ceramic preparation caps, but they are not absolutely necessary for a successful MIMI® treatment. After the gentle implantation and cementation, they will allow for compensation of insertion divergences still in the same session This has always been a dream for a dentist: you insert the implant. Then, the treatment is almost the same as for a natural tooth. After the impression is taken, the temporary restoration is fitted, and the first bite registration is taken. With this registration, the laboratory is informed of how the patient bites his/her teeth together (occlusion). The dental technician also considers the stump in the impression as a natural tooth. It is cast with super hard plaster. The preparation margin can be done under hygienic conditions and supra-gingivally (over the gingiva margin). External micro-movements are to be excluded through (preferably) splinted temporary restorations. Participation of the patient is absolutely necessary. The patient should eat soft food without sharp edges. He/she should practice good oral hygiene and eventually rinse his/her mouth with chlorhexidine.



Four days after the MIMI® implantation, the framework was fitted. The framework can be made of a metal alloy, but it should be the miniature form of the later prosthodontic restoration. Four days after a second bite registration was taken with the framework, which was passively fitted on the implants (in this case: on the Champions®), the prosthodontic restoration was finally fitted with standard Glass Ionomer Base Cement. Pronounced occlusal cusp and fissure reliefs (which adolescents may have) are to be avoided because of excessive lateral movements and shear forces.
In current medicine, there are a lot of possibilities, but not everything is necessary and reasonable!